
Understanding why rest isn't always the best medicine
Chronic pain conditions and acute pain can be confusing; sometimes, it appears without warning, lingers for weeks, and refuses to follow logic. Many people assume that chronic pain or acute pain always means injury or that complete rest is the safest solution.
But modern pain science tells a very different story.
As physiotherapists, one of our main roles is to help people understand what the pain really means and to shift the mindset from “protect and rest” to “move and adapt.”
Let’s take a look some of the most common chronic pain and acute pain myths and explore why gentle, guided movement is often the key to true recovery.
Myth 1: Pain Always Means Damage
This is one of the most deeply ingrained beliefs and one of the most misleading. Chronic pain conditions and acute pain are not always direct measures of tissue damage. It’s your body’s protective alarm system designed to keep you safe.
Think of it this way: if pain always matched damage, a paper cut would barely register, and a disc bulge on MRI would always hurt. But that’s not what happens. You can have severe pain from something minor, or little to no pain despite visible changes on imaging.
Your nervous system constantly scans for “threats.” It combines information from your body, environment, emotions, and even memories to decide whether to create a pain response. In some cases, like with chronic pain or long-standing pain, that system becomes overprotective. It rings the alarm even when no real tissue danger exists.
The goal of rehab, then, is not just to “fix what’s broken,” but to retrain that alarm system to respond appropriately again.
Myth 2: I Should Rest Completely Until the Pain is Gone
Rest feels safe and in the very early stage of an injury, it can be useful to let inflammation settle. But beyond the first few days, complete rest often does more harm than good.
Here’s why:
- Muscles weaken quickly. You can lose strength and muscle mass within a week of total inactivity.
- Joints stiffen. Lack of movement limits nutrient flow to cartilage and connective tissue.
- Healing slows down. Blood flow and tissue remodelling rely on movement and light loading.
- Fear increases. The longer you avoid movement, the more your brain associates it with danger.
Instead of strict rest, physiotherapists use the principle of “relative rest.” That means you modify or reduce the load, but you keep moving in some way.
For example, after a knee injury, you might avoid running or deep squats for a while, but you can still do gentle range-of-motion exercises, isometric contractions, or pool walking. This keeps your body strong, improves circulation, and maintains confidence in movement.
Vuurberg et al. (2018) reported that early functional treatment including early loading and movement is associated with lower re-injury rates and a faster return to sport and daily activities after a common lateral ankle sprain.
Movement is not just exercises it’s a neurological message that says “it’s safe to move again.”
Myth 3: My MRI looks bad, so I must be Broken
Modern imaging is an amazing diagnostic tool, but it often causes unnecessary worry.
Multiple studies show that people with no pain at all often have “degenerative” findings on scans such as disc bulges, tears, or cartilage wear.
Brinjikji et al. (2015) demonstrated that disc-related ‘pathological’ findings are extremely common even in people with no symptoms at all. This highlights that many imaging changes such as disc bulges or degeneration are often a normal part of ageing rather than a direct source of pain.
For example:
- Around 60% of people over 40 have disc bulges on MRI without symptoms.
- Many athletes show meniscus or rotator cuff changes despite full function and no pain.
Why? Because structural changes are a normal part of ageing and adaptation. Your body remodels constantly, just like your skin forms calluses from friction.
Pain depends more on sensitivity and load tolerance than on what’s visible on a scan. So instead of chasing a “perfect MRI,” rehab focuses on improving movement, strength, and confidence, the things that actually change your pain experience.
Myth 4: Pain Flare-Ups Mean I’m Getting Worse
A flare-up of a chronic pain condition or acute pain can feel discouraging, but it’s rarely a sign of damage or regression. Interestingly, pain can naturally fluctuate depending on stress, sleep, load, and even mood.
Think of a flare-up as feedback your body telling you it’s temporarily sensitive. If you interpret that signal calmly, make small adjustments, and continue moving within tolerance, your baseline improves over time.
Progress isn’t always a straight line. But each flare-up is a chance to learn how your system responds and build resilience for next time.
Putting it all Together
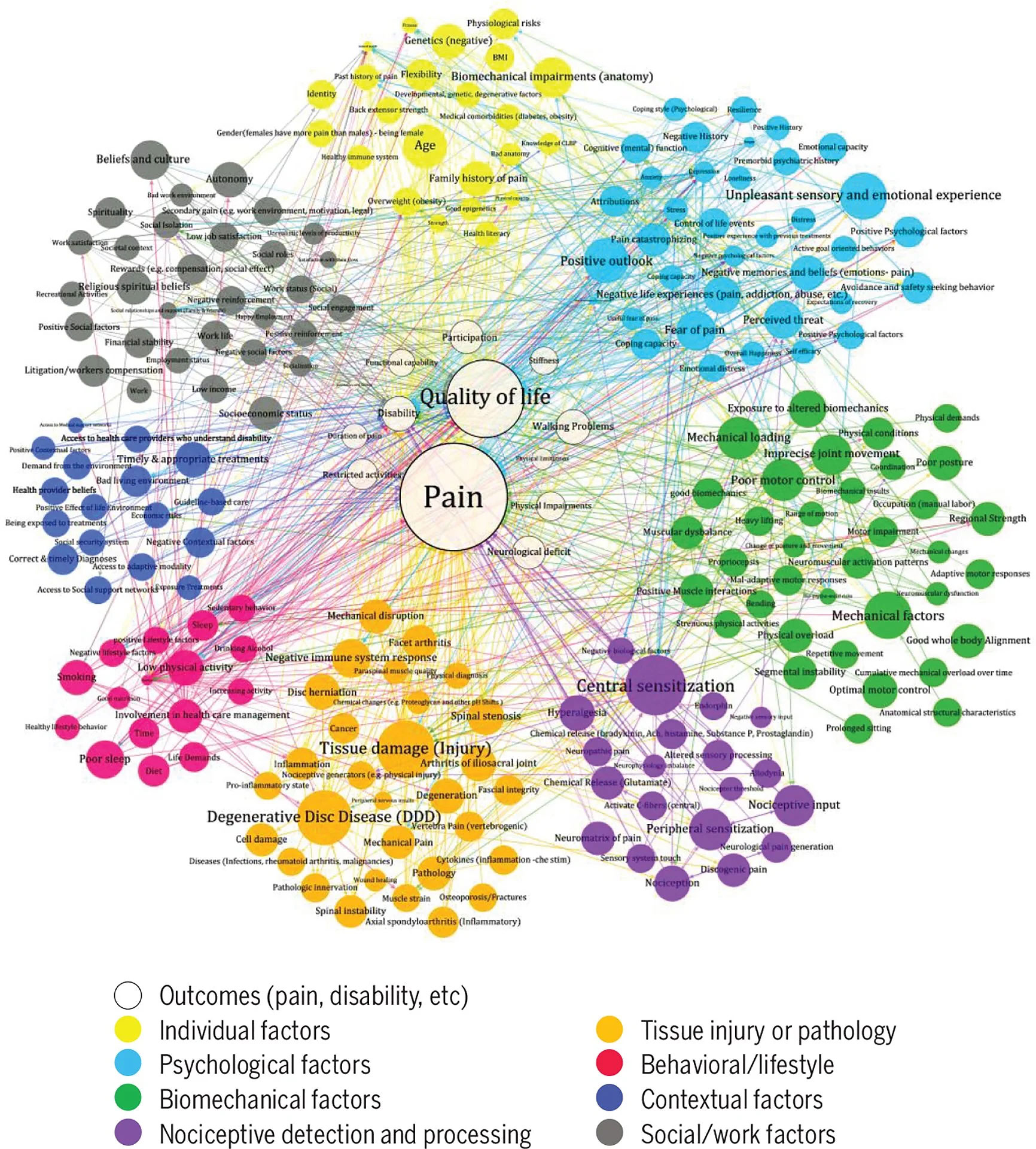
Pain is real, but it’s also complex. It’s influenced by biology, psychology, social and environment, not just tissue damage.
That’s why the best recovery plans for chronic pain conditions and acute pain combine education, movement, and support rather than just rest or medication.
If you’re dealing with ongoing pain:
- Stay curious, not fearful. Understanding your pain gives you control.
- Keep moving safely. Modify, don’t stop. Use the “relative rest” principle.
- Seek guidance. A physio can help tailor movement and loading for your situation.
- Track progress, not perfection. Flares are part of the journey.
Your body is strong, adaptable, and designed to heal. The more you move with confidence, the more your system learns that it’s safe again.
References:
Cholewicki, J., Breen, A., Popovich Jr, J. M., Reeves, N. P., Sahrmann, S. A., Van Dillen, L. R., … & Hodges, P. W. (2019). Can biomechanics research lead to more effective treatment of low back pain? A point-counterpoint debate. journal of orthopaedic & sports physical therapy, 49(6), 425-436.
Vuurberg, G., Hoorntje, A., Wink, L. M., Van Der Doelen, B. F., Van Den Bekerom, M. P., Dekker, R., … & Kerkhoffs, G. M. (2018). Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline. British journal of sports medicine, 52(15), 956-956.
Brinjikji, W., Diehn, F. E., Jarvik, J. G., Carr, C. M., Kallmes, D. F., Murad, M. H., & Luetmer, P. H. (2015). MRI findings of disc degeneration are more prevalent in adults with low back pain than in asymptomatic controls: a systematic review and meta-analysis. American Journal of Neuroradiology, 36(12), 2394-2399.