In this post, we’ll cover all the key points about Achilles tendinopathy, including its pathology, diagnosis, assessment, and management. Let’s dive in!
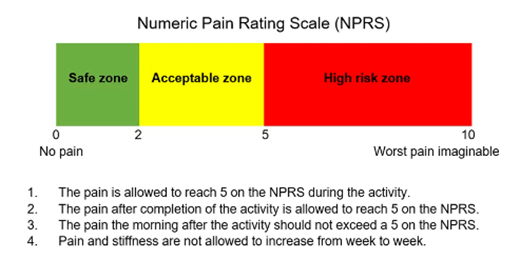
What Is Achilles Tendinopathy?
Achilles tendinopathy occurs when the collagen fibres in the Achilles tendon become disorganised. Imagine the tendon like a bundle of uncooked spaghetti, with each strand representing a collagen fibre (photo below). Normally, these fibres line up neatly, working together to transmit force from your muscles to your bones, helping you move.
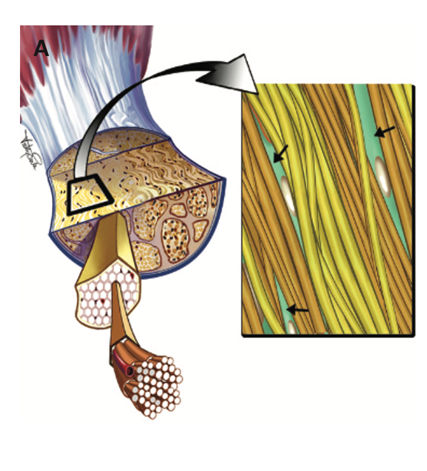
However, when the tendon is overloaded, things start to go wrong. Some fibres no longer run parallel, and others might be lost altogether, making the tendon less effective at transmitting force. As a result, activities like walking, running, or jumping become more difficult.
How Is Achilles Tendinopathy Diagnosed?
Achilles tendinopathy is typically diagnosed based on your symptoms. Localised pain, swelling, and reduced function are key signs (Malliaras, 2022). There are two types of Achilles tendinopathy: insertional (near the heel) and mid-portion (further up the tendon) (photo below). The location of your pain can help determine which type you may have.

Although an ultrasound can be used to diagnose this condition, it’s not always necessary. Clinical assessment is usually enough. In fact, ultrasound findings alone can be misleading, as many people without pain also show tendon changes on scans (Lieberthal et al., 2019). So, the focus should be on your symptoms, not just what the scan shows.
Achilles tendinopathy often occurs after a sudden increase in activity, like when people start running after a break, or athletes return to sport after time off. Lifestyle factors like diabetes, menopause, smoking, and poor sleep can also increase your risk.
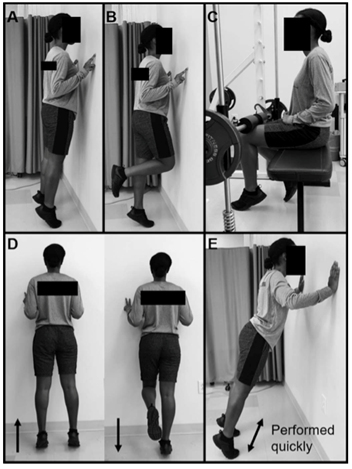
What to Expect During a Physiotherapy Assessment
When you come to our clinic, there are six key things we’ll assess:
1. Observation – We’ll look for visible swelling in your Achilles tendon.
2. Palpation – We’ll gently press on your tendon to see if it reproduces your pain.

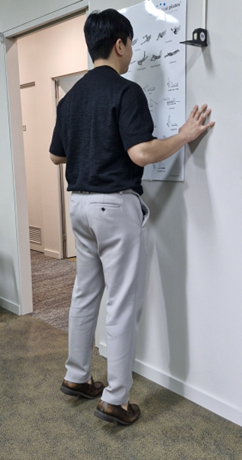
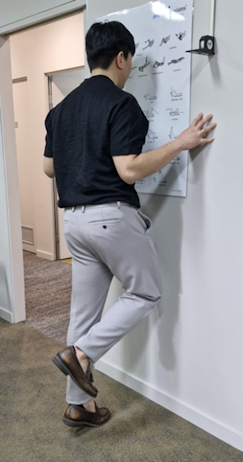
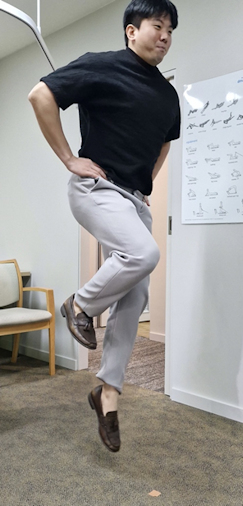
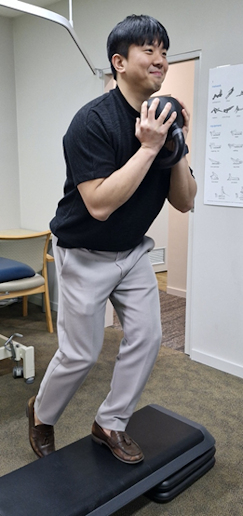
3. Capability Assessments – We’ll check how much load your tendon can handle. This is crucial for planning your treatment.
It would normally include: